AI cardiovascular quantification · Breast arterial calcification
Read the heart in the mammogram she already took.
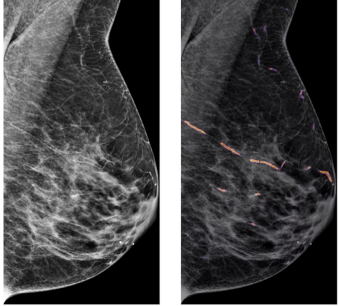
Avera turns the most routine scan in women's medicine into a quantitative cardiovascular signal. The only model that measures breast arterial calcification in absolute mm², across every major scanner.
BAC score = 37.61 mm²
Heatmap overlay